

Chronic pain and women’s health: innovations to track in 2026
FFHi Brief: A deep dive into the context of women's chronic pain and the companies innovating in the space.


Chronic pain is one of the most common reasons women seek medical care — yet it remains one of the most under-researched and poorly treated areas of healthcare.
While around 70% of people living with chronic pain are women, the systems of diagnosis, research and treatment have historically been built around a male baseline. The result? Women’s pain is still too often delayed, dismissed or inadequately managed.
This deep dive FFHi brief, written by women’s health strategist Anastasiya Markvarde, explores the structural drivers behind the gap — and spotlights the startups and innovators building new tools to better measure, track and manage pain. These emerging approaches signal the beginning of a long-overdue shift in how chronic pain in women is understood and treated.
Research and clinical biases in chronic pain
Historically, we haven’t studied women’s pain.
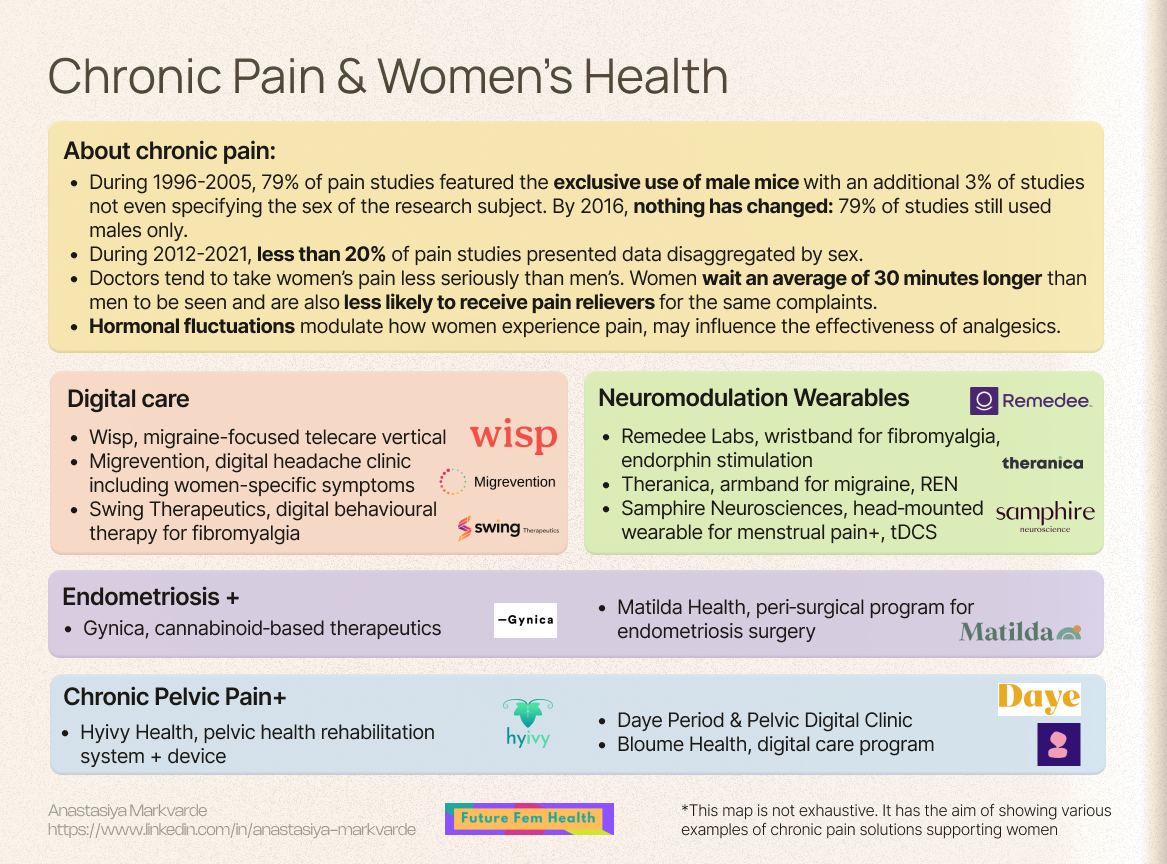
A review of preclinical research published in the journal Pain from 1996- 2005 showed that 79% of studies featured the exclusive use of male mice, with an additional 3% of studies not even specifying the sex of the research subject. Fast forward another decade and a similar review of Pain papers published in 2016 showed that nothing had changed over 20 years: 79% of studies still used males only. A systematic review of publications in Pain from 2012-2021 concluded that less than 20% presented data disaggregated by sex.
The result of this lack of research is that pain science has struggled to explain - let alone treat - the kinds of chronic, fluctuating pain patterns that disproportionately affect women.
Women generally experience more recurrent pain, more severe pain and longer lasting pain than men. These biological differences directly affect which treatments work, which fail, and which side effects women experience. Their pain response to drugs may differ. For example, opioids tend to have less effect on women, and we assume it’s because women regulate pain through partly different biological mechanisms, involving distinct hormone effects, immune pathways, neural circuits, and even endogenous analgesic systems. In this study in PNAS Nexus the researchers measured the effect of meditation on pain. It turned out that when men used the meditation technique to reduce their pain, that pain relief was mainly produced by their own internal opioid system (their brain’s natural morphine‑like chemicals), but when women did the same, their pain relief came from other biological pathways instead of those natural opioids.
Women with pain also face care biases. Doctors tend to take women’s pain less seriously than men’s, and are likely to assume that female patients are exaggerating their discomfort. The international analysis in PNAS showed that clinicians treat women and men differently when they show up at a hospital with pain. Women wait an average of 30 minutes longer than men to be seen and are also less likely to receive pain relievers for the same complaints.
In addition, hormonal fluctuations, particularly changes in estrogen and progesterone, significantly modulate how women experience pain throughout their lives, including during the menstrual cycle, pregnancy, and menopause. It’s also recognised that hormonal changes may significantly influence pain thresholds and the effectiveness of analgesics and anesthetics. However, current research in the area is not advanced enough in order to tailor pain treatments to women based on their hormonal levels and status.
Conditions behind chronic pain
There are a number of common chronic pain-related conditions which are more prevalent in women than men, such as migraine, fibromyalgia, chronic pelvic pain or autoimmune diseases. A few women-only conditions also cause chronic pain, for example, endometriosis.
The research and care gaps detailed above are most visible in these types of conditions that disproportionately affect women - many of which are still under-diagnosed, under-treated or both.
Migraine
Narrative and epidemiological reviews show that global migraine prevalence is about 20.7% in women vs. 9.7% in men. After puberty, migraine becomes 3 - 4 times more common in women. Women also report longer attacks, greater disability, higher recurrence, and longer recovery than men. As touched upon above, hormonal fluctuations in women - especially estrogen fluctuations - were found to be associated with migraines. Hormone‑linked migraines intensify before menstruation, around reproductive milestones such as pregnancy and postpartum, and often worsen during perimenopause when estrogen levels start fluctuating and eventually drop.
Fibromyalgia
Fibromyalgia is a long‑term pain disorder, thought to be caused by the nervous system becoming overly sensitive, causing widespread musculoskeletal pain, fatigue, and sleep disturbances. It affects up to 2 -5% of the population and shows a female predominance of 75 -90% in many clinical samples. A 2023 scoping review estimated that 80 - 96% of diagnosed fibromyalgia cases are female, even if population‑based studies using modern criteria suggest a prevalence of roughly 4% in women versus 1.4% in men. Similarly to migraine, higher prevalence of fibromyalgia in women is attributed to hormonal changes and difference in how women’s bodies manage stress responses.
Endometriosis and chronic pelvic pain
Endometriosis affects around 10% of reproductive‑age women globally and takes on average 7 years or more to diagnose. Endometriosis has historically been treated as a gynaecologic condition rather than a chronic pain disorder since it impacts quality of life much beyond chronic pain, and is associated with systemic comorbidities including autoimmune and metabolic conditions, infertility or subfertility. This has shaped both diagnostic pathways and innovation priorities. Yet pain is also a large part of endometriosis. Chronic pelvic pain affects roughly one in five women, and a substantial fraction but not the majority of chronic pelvic pain is attributable to endometriosis, with the remainder linked to other gynecologic, urologic, gastrointestinal, musculoskeletal, neuropathic, or centrally mediated causes.
Diagnostic delays of these conditions are driven by normalisation of severe period pain, limited awareness among clinicians, reliance on surgery for definitive diagnosis, and communication gaps where numeric pain scales fail to capture the full impact on daily life. There is also a lack of validated non‑invasive diagnostics and pain‑focused therapies for endometriosis and chronic pelvic pain, even if novel solutions are emerging. For example, new daily combined hormonal treatments were approved in the UK in 2025 as more convenient options for endometriosis pain management.
Autoimmune diseases
Many autoimmune diseases that are more common in women also cause significant chronic pain, such as:
Rheumatoid arthritis, ratio women/men is 3:1. Causes chronic inflammatory joint pain, swelling, and stiffness, especially in hands and feet.
Lupus, ratio women/men is 9:1. Leads to joint and muscle pain, headaches, chest pain, and widespread inflammatory pain.
Sjögren’s syndrome, ratio women/men is 9:1. Causes joint pain, muscle aches, neuropathic‑type burning or tingling, and painful dryness of eyes, mouth, and sometimes vaginal tissue.
Multiple sclerosis, ratio women/men is 9:1. Can cause neuropathic pain, muscle cramps, and painful spasticity.
Innovations supporting chronic pain women patients
Below are some examples of startups supporting patients with chronic pain depending on the condition. While not all of them target women only, these solutions address women-specific symptoms or have done studies focused on women. They reflect a broader shift towards pain care that accounts for hormonal dynamics, life stage and female-dominant conditions.
A growing wave of startups are attempting to close the care gap through digital-first, home-based and neuromodulation-driven approaches.
Digital care:
Women’s telehealth provider Wisp launched a new, migraine-dedicated care vertical in 2025, ranging from online consults and prescribing therapies to on-going follow-up and longitudinal care for patients.
Migrevention is a women-founded digital headache clinic comprising a tracking app and remote nurse counselling. The app allows users to log headache frequency, intensity, medication usage, and potential triggers like hormonal fluctuations related to the menstrual cycle app‑based headache.
Newly funded Danish start-up Hemi Health also tackles migraine and concussion care, and women make up 80% of their patient base.
Stanza by Swing Therapeutics developed a mobile acceptance and commitment therapy app for fibromyalgia, which has received FDA De Novo authorization. While Swing DTx and the virtual clinic are available to all genders, fibromyalgia is predominantly diagnosed in women, and the trial to evaluate Stanza safety and efficacy had 93% women participants.
Neuromodulation wearables:
Nerivio by Theranica is an FDA‑cleared remote electrical neuromodulation (REN) armband for acute and preventive migraine treatment that can be used at home. About 66% of Nerivio users achieve significant pain relief, and around 37% achieve pain freedom in clinical studies. While indicated for migraine in adolescents and adults of all genders, Theranica ran specific studies in menstrual migraine and in pregnant women, explicitly targeting women‑specific scenarios and safety questions.
Remedee Labs developed a personal endorphin‑stimulation wearable which became the first dedicated technological solution for fibromyalgia to receive a medical device status in Europe. 95% of patients in the clinical trial of Remedee Labs were women. Over half of patients (53%) went from severe to moderate intensity of fibromyalgia, and the improvement remained in place at 6 months.
Nettle by Samphire Neurosciences is a head‑mounted wearable that delivers non‑invasive transcranial direct current stimulation (tDCS) to brain regions involved in pain perception and mood regulation. It is specifically designed for menstrual pain, PMS/PMDD mood symptoms, and related conditions such as endometriosis and uterine fibroids. Nettle’s data show that 72% of users experienced reduced pain within one cycle, 73% reported improved mood, and 69% reported reduced bloating, based on self‑reported outcomes from their initial user cohort and WIND trial data.
Endometriosis:
Gynica is developing cannabinoid‑based therapeutics for chronic menstrual pain and dyspareunia, including pain associated with endometriosis, based on research into the endocannabinoid system in the female reproductive tract.
Chugai and Biofourmis entered into the partnership to build a digital solution for objective pain assessment in endometriosis, using a clinical‑grade wearable biosensor and AI algorithms on Biofourmis’ Biovitals platform. The project was originally announced in 2020 with a more extended agreement in 2023, however, no public updates on the progress have emerged since then.
Matilda Health offers an 8‑week digital peri‑surgical program for endometriosis surgery (4 weeks pre‑op + 4 weeks post‑op), combining education, physiotherapy, psychological support, and lifestyle guidance to reduce pain, complications, and recovery time. In general, patients receiving preoperative care for endometriosis surgery report about 17% lower pain intensity 48 hours after surgery, and pre-rehabilitation is an important component of the rehabilitation process often overlooked by healthcare systems.
Chronic pelvic pain:
Bloume is developing an AI‑powered digital solution targeting vulvodynia, endometriosis‑related pain, and broader chronic pelvic pain. Biopsychosocial digital program combining psychological support, pelvic floor physiotherapy, and sex/relationship therapy within one platform.
Daye has launched a Period & Pelvic Pain Clinic, using clinically validated questionnaires and algorithms to screen for endometriosis and other gynecologic causes, then route to tele‑gyn or specialist care.
Hyivy Health is advancing Floora as part of a smart, multi-therapy pelvic health rehabilitation system that combines an intravaginal device with app guidance and clinician software to support at-home pelvic rehabilitation. The system integrates controlled dilation, thermal modulation, and embedded sensors with real-time data tracking and remote clinician connectivity. It is being developed to improve treatment of pelvic floor dysfunction and related chronic pelvic pain, with ongoing clinical research into its broader therapeutic value.
There are also innovative neuromodulation approaches emerging for autoimmune-related pain and inflammation. SetPoint Medical is developing the SetPoint System, an implantable vagus-nerve stimulation device designed to modulate inflammatory pathways in rheumatoid arthritis and other autoimmune diseases, with the goal of reducing disease activity and associated symptoms such as joint pain and swelling in patients who do not respond adequately to biologic therapies. Boomerang Medical, a women-led bioelectronic medicine startup, is advancing neuromodulation approaches for inflammatory bowel diseases such as Crohn’s disease and ulcerative colitis, aiming to alleviate symptom burden - including chronic abdominal pain and cramping - by modulating neural pathways involved in gut and immune function.
Another approach to chronic pain is brain retraining - teaching the nervous system to reinterpret pain signals as less threatening, using tools like cognitive behavioral therapy, somatic tracking, and emotional regulation exercises. An example of a startup offering this kind of support is Curable. They offer digital programs that combine education on modern pain neuroscience with guided practices to “retrain your brain” and have reported clinically significant improvements in conditions like back pain and migraine, although results vary by individual and are strongest when people engage consistently over time.
New methods to bridge the chronic pain gap for women are emerging. For example, researchers at Tufts University are developing novel approaches to quantifying chronic pain in women to reduce reliance on subjective scores. The aim of the research is to choose the five most reliable biomarkers linked to pain out of the 30 analyzed, so that these can be monitored in real time using a portable device, ultimately leading to better pain management in women.
Conclusion
Women continue to bear a disproportionate burden of chronic pain, yet much of our research, measurement, and treatment infrastructure was built around male bodies and male data.
Clearly, our research and clinical standards in chronic pain treatment and management should include women-specific studies and measurements. But what’s changing ahead of this new research is new ways of seeing pain and treating it. Emerging innovations, from neuromodulation wearables to digital pain clinics, have created new opportunities for women to track and manage their pain accounting for female biology and hormonal fluctuations.
Now, the next phase of progress will depend on whether these innovations move from individual solutions to standard care - and whether healthcare systems are willing to acknowledge women’s pain and redesign pain management around women’s biology, rather than treating it as a deviation from the norm.
This article was written for FutureFemHealth by women’s health strategist Anastasiya Markvarde.
You might also like our other FFHi briefs:
Menstrual blood diagnostics in 2026: what's changing - and what we're tracking

For years, small groups of determined researchers, clinicians and founders have been working to destigmatise and normalise menstrual blood as a source of usable health data.
Women’s hormonal healthtech: what to expect from the fast-growing innovation landscape in 2026

A guest post by Anastasiya Markvarde
 | A guest post by
|